
Relationship between White Matter Alterations and Pathophysiological Symptoms in Patients with Ultra-High Risk of Psychosis, First-Episode, and Chronic Schizophrenia

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Assessments
2.3. Image Acquisition
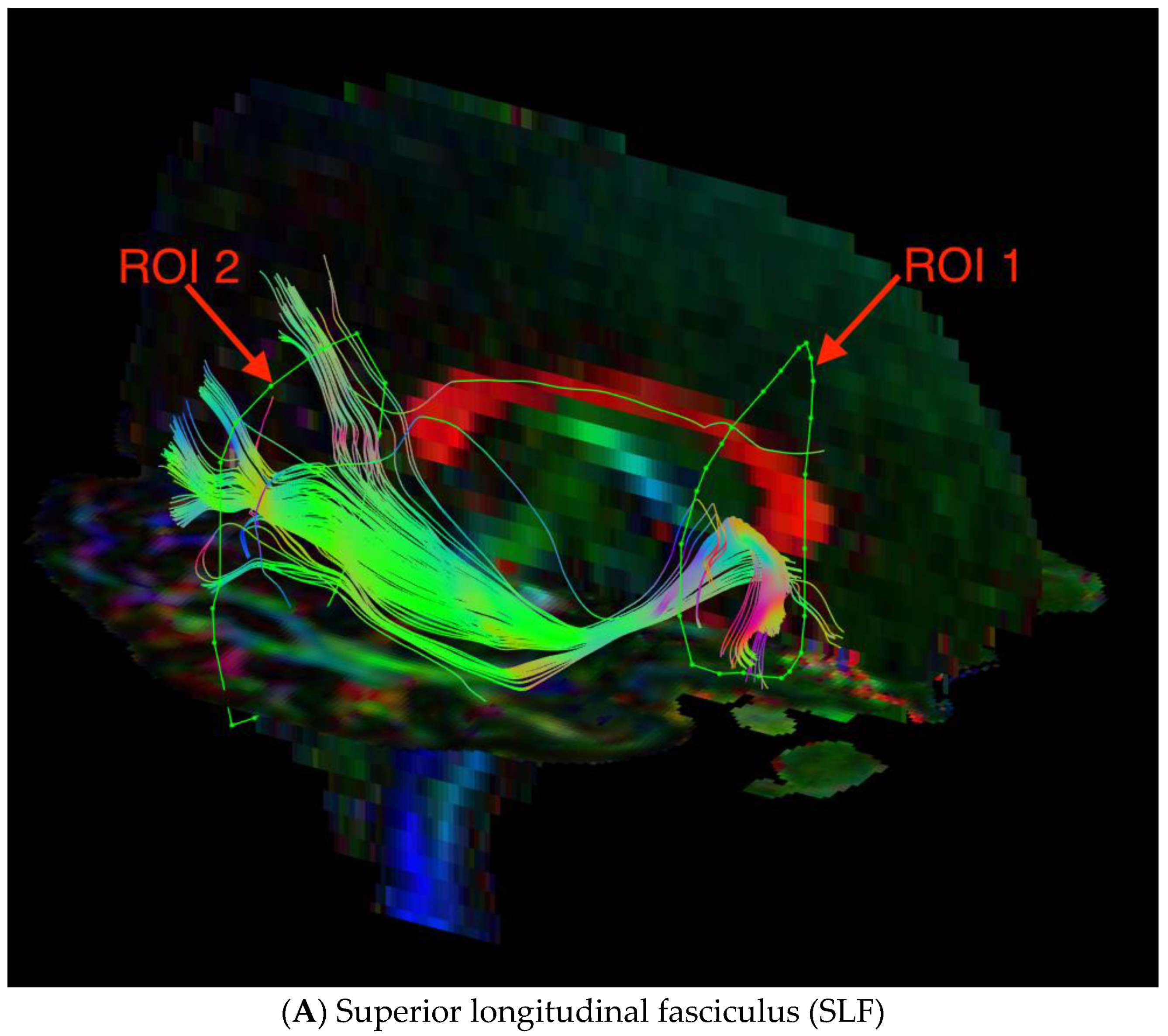
2.4. Image Processing and Quality
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Differences in DTI Measures
3.3. Differences in Psychopathological Dimensions
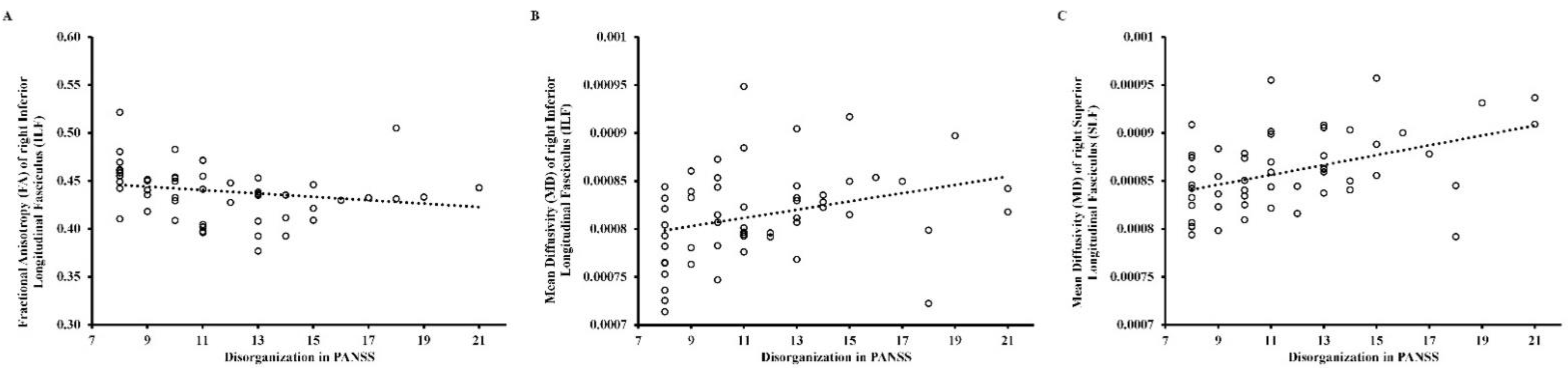
3.4. Relationship between DTI Measures and Psychopathological Dimensions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tyburski, E.; Pełka-Wysiecka, J.; Mak, M.; Samochowiec, A.; Bieńkowski, P.; Samochowiec, J. Neuropsychological profile of specific executive dysfunctions in patients with deficit and non-deficit schizophrenia. Front. Psychol. 2017, 8, 1459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fioravanti, M.; Bianchi, V.; Cinti, M.E. Cognitive deficits in schizophrenia: An updated metanalysis of the scientific evidence. BMC Psychiatry 2012, 12, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Os, J.; Kapur, S. Schizophrenia. Lancet 2009, 374, 635–645. [Google Scholar] [CrossRef]
- Harvey, P.D.; Heaton, R.K.; Carpenter, W.T., Jr.; Green, M.F.; Gold, J.M.; Schoenbaum, M. Functional impairment in people with schizophrenia: Focus on employability and eligibility for disability compensation. Schizophrenia Res. 2012, 140, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Charrier, N.; Chevreul, K.; Durand-Zaleski, I. Le coût de la schizophrénie: Revue de la littérature internationale. L'Encéphale 2013, 39, S49–S56. [Google Scholar] [CrossRef] [PubMed]
- Crow, T.J. The Two-Syndrome concept: Origins and current status. Schizophr. Bull. 1985, 11, 471–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The Positive and Negative Syndrome Scale (PANSS) for schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef]
- Andreasen, N.C. The Scale for the Assessment of Positive Symptoms (SAPS); Univ. Iowa: Iowa City, 1984. [Google Scholar]
- Andreasen, N.C. The Scale for the Assessment of Negative Symptoms (SANS): Conceptual and theoretical foundations. Br. J. Psychiatry Suppl. 1989, 7, 49–58. [Google Scholar] [CrossRef]
- Horan, W.P.; Kring, A.M.; Gur, R.E.; Reise, S.P.; Blanchard, J.J. Development and psychometric validation of the Clinical Assessment Interview for Negative Symptoms (CAINS). Schizophrenia Res. 2011, 132, 140–145. [Google Scholar] [CrossRef] [Green Version]
- Kirkpatrick, B.; Strauss, G.P.; Nguyen, L.; Fischer, B.A.; Daniel, D.G.; Cienfuegos, A.; Marder, S.R. The Brief negative symptom scale: Psychometric properties. Schizophr. Bull. 2011, 37, 300–305. [Google Scholar] [CrossRef]
- Shafer, A.; Dazzi, F. Meta-analysis of the positive and Negative Syndrome Scale (PANSS) factor structure. J. Psychiatr. Res. 2019, 115, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, P.; Deste, G.; Smieskova, R.; Barlati, S.; Yung, A.; Howes, O.; Stieglitz, R.-D.; Vita, A.; McGuire, P.; Borgwardt, S. Cognitive Functioning in Prodromal Psychosis. Arch. Gen. Psychiatry 2012, 69, 562–571. [Google Scholar] [CrossRef] [PubMed]
- Bora, E.; Murray, R. Meta-Analysis of cognitive deficits in Ultra-high Risk to psychosis and first-episode psychosis: Do the cognitive deficits progress over, or after, the onset of psychosis? Schizophr. Bull. 2014, 40, 744–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Häfner, H.; Löffler, W.; Maurer, K.; Hambrecht, M.; Der Heiden, W.A. Depression, negative symptoms, social stagnation and social decline in the early course of schizophrenia. Acta Psychiatr. Scand. 1999, 100, 105–118. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, P.; Bonoldi, I.; Yung, A.R.; Borgwardt, S.; Kempton, M.J.; Valmaggia, L.; Barale, F.; Caverzasi, E.; McGuire, P. Predicting psychosis. Arch. Gen. Psychiatry 2012, 69, 220–229. [Google Scholar] [CrossRef] [Green Version]
- O'Donoghue, B.; Nelson, B.; Yuen, H.P.; Lane, A.; Wood, S.; Thompson, A.; Lin, A.; McGorry, P.; Yung, A.R. Social environmental risk factors for transition to psychosis in an Ultra-High Risk population. Schizophr. Res. 2015, 161, 150–155. [Google Scholar] [CrossRef]
- Auquier, P.; Lançon, C.; Rouillon, F.; Lader, M.; Holmes, C. Mortality in schizophrenia. Pharmacoepidemiol. Drug Saf. 2006, 15, 873–879. [Google Scholar] [CrossRef]
- Addington, J.; Cornblatt, B.A.; Cadenhead, K.S.; Cannon, T.D.; McGlashan, T.H.; Perkins, D.O.; Seidman, L.J.; Tsuang, M.T.; Walker, E.F.; Woods, S.W.; et al. At clinical high risk for psychosis: Outcome for nonconverters. Am. J. Psychiatry 2011, 168, 800–805. [Google Scholar] [CrossRef] [Green Version]
- Miller, T.J.; McGlashan, T.H.; Woods, S.W.; Stein, K.; Driesen, N.; Corcoran, C.; Hoffman, R.; Davidson, L. Symptom assessment in schizophrenic prodromal states. Psychiatr. Q. 1999, 70, 273–287. [Google Scholar] [CrossRef]
- Yung, A.R.; Yuen, H.P.; McGorry, P.D.; Phillips, L.; Kelly, D.; Dell’Olio, M.; Francey, S.M.; Cosgrave, E.M.; Killackey, E.; Stanford, C.; et al. Mapping the onset of psychosis: The comprehensive assessment of at-risk mental states. Aust. N. Z. J. Psychiatry 2005, 39, 964–971. [Google Scholar] [CrossRef]
- Andreasen, N.C. Schizophrenia: The fundamental questions. Brain Res. Rev. 2000, 31, 106–112. [Google Scholar] [CrossRef]
- Friston, K.; Brown, H.R.; Siemerkus, J.; Stephan, K.E. The dysconnection hypothesis. Schizophr. Res. 2016, 176, 83–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Fan, L.; Qiu, C.; Jiang, T. Prefrontal cortex and the dysconnectivity hypothesis of schizophrenia. Neurosci. Bull. 2015, 31, 207–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephan, K.E.; Friston, K.; Frith, C. Dysconnection in schizophrenia: From abnormal synaptic plasticity to failures of self-monitoring. Schizophr. Bull. 2009, 35, 509–527. [Google Scholar] [CrossRef] [Green Version]
- Alexander, A.L.; Lee, J.E.; Lazar, M.; Field, A.S. Diffusion tensor imaging of the brain. Neurotherapeutics 2007, 4, 316–329. [Google Scholar] [CrossRef] [Green Version]
- Smith, R.E.; Tournier, J.-D.; Calamante, F.; Connelly, A. Anatomically-Constrained tractography: Improved diffusion MRI streamlines tractography through effective use of anatomical information. NeuroImage 2012, 62, 1924–1938. [Google Scholar] [CrossRef] [PubMed]
- Jeurissen, B.; Leemans, A.; Tournier, J.-D.; Jones, D.K.; Sijbers, J. Investigating the prevalence of complex fiber configurations in white matter tissue with diffusion magnetic resonance imaging. Hum. Brain Mapp. 2013, 34, 2747–2766. [Google Scholar] [CrossRef] [PubMed]
- Tournier, J.-D.; Calamante, F.; Connelly, A. Robust determination of the fibre orientation distribution in diffusion MRI: Non-negativity constrained super-resolved spherical deconvolution. NeuroImage 2008, 35, 1459–1472. [Google Scholar] [CrossRef]
- Kelly, S.; Jahanshad, N.; Zalesky, A.; Kochunov, P.; Agartz, I.; Alloza, C.; Andreassen, O.A.; Arango, C.; Banaj, N.; Bouix, S.; et al. Widespread white matter microstructural differences in schizophrenia across 4322 individuals: Results from the ENIGMA schizophrenia DTI working group. Mol. Psychiatry 2018, 23, 1261–1269. [Google Scholar] [CrossRef] [Green Version]
- Alterations of cerebral white matter structure in psychosis and their clinical correlations: A systematic review of Diffusion Tensor Imaging studies. Riv. Psichiatr. 2017, 52, 49–66. [CrossRef]
- Podwalski, P.; Szczygieł, K.; Tyburski, E.; Sagan, L.; Misiak, B.; Samochowiec, J. Magnetic resonance diffusion tensor imaging in psychiatry: A narrative review of its potential role in diagnosis. Pharmacol. Rep. 2021, 73, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Waszczuk, K.; Rek-Owodziń, K.; Tyburski, E.; Mak, M.; Misiak, B.; Samochowiec, J. Disturbances in white matter integrity in the ultra-high-risk psychosis state—A systematic review. J. Clin. Med. 2021, 10, 2515. [Google Scholar] [CrossRef] [PubMed]
- Mubarik, A.; Tohid, H. Frontal lobe alterations in schizophrenia: A review. Trends Psychiatry Psychother. 2016, 38, 198–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turetsky, B.; Cowell, P.E.; Gur, R.C.; Grossman, R.I.; Shtasel, D.L.; Gur, R.E. Frontal and temporal lobe brain volumes in schizophrenia. Arch. Gen. Psychiatry 1995, 52, 1061–1070. [Google Scholar] [CrossRef]
- Nakajima, R.; Kinoshita, M.; Shinohara, H.; Nakada, M. The superior longitudinal fascicle: Reconsidering the fronto-parietal neural network based on anatomy and function. Brain Imaging Behav. 2020, 14, 2817–2830. [Google Scholar] [CrossRef]
- Chawla, N.; Deep, R.; Khandelwal, S.K.; Garg, A. Reduced integrity of superior longitudinal fasciculus and arcuate fasciculus as a marker for auditory hallucinations in schizophrenia: A DTI tractography study. Asian J. Psychiatry 2019, 44, 179–186. [Google Scholar] [CrossRef]
- Sato, Y.; Sakuma, A.; Ohmuro, N.; Katsura, M.; Abe, K.; Tomimoto, K.; Iizuka, K.; Ito, F.; Tomita, H.; Matsumoto, K. Relationship between white matter microstructure and hallucination severity in the early stages of psychosis: A diffusion tensor imaging study. Schizophr. Bull. Open 2021, 2, 1–11. [Google Scholar] [CrossRef]
- Shergill, S.S.; Kanaan, R.A.; Chitnis, X.A.; O’Daly, O.; Jones, D.K.; Frangou, S.; Williams, S.C.; Howard, R.J.; Barker, G.J.; Murray, R.M.; et al. A diffusion tensor imaging study of fasciculi in schizophrenia. Am. J. Psychiatry 2007, 164, 467–473. [Google Scholar] [CrossRef]
- Ashtari, M.; Cottone, J.; Ardekani, B.A.; Cervellione, K.; Szeszko, P.R.; Wu, J.; Chen, S.; Kumra, S. Disruption of white matter integrity in the inferior longitudinal fasciculus in adolescents with schizophrenia as revealed by fiber tractography. Arch. Gen. Psychiatry 2007, 64, 1270–1280. [Google Scholar] [CrossRef] [Green Version]
- Herbet, G.; Zemmoura, I.; Duffau, H. Functional anatomy of the inferior longitudinal fasciculus: From historical reports to current hypotheses. Front. Neuroanat. 2018, 12, 77. [Google Scholar] [CrossRef] [Green Version]
- Chan, W.-Y.; Yang, G.-L.; Chia, M.-Y.; Lau, I.-Y.; Sitoh, Y.-Y.; Nowinski, W.L.; Sim, K. White matter abnormalities in first-episode schizophrenia: A combined structural MRI and DTI study. Schizophr. Res. 2010, 119, 52–60. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). The ICD-10 Classification of Mental and Behavioural Disorders; World Health Organization: Geneva, Switzerland, 1993. [Google Scholar]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Balker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. 20), 22–33. [Google Scholar] [PubMed]
- Hall, R.C. Global assessment of functioning: A modified scale. Psychosomatics 1995, 36, 267–275. [Google Scholar] [CrossRef]
- Leemans, A.; Jeurissen, B.; Sijbers, J.; Jones, D.K. ExploreDTI: A graphical toolbox for processing, analyzing, and visualizing diffusion MR data. Proc. Int. Soc. Magn. Reson. Med. 2009, 17, 3537. [Google Scholar]
- Hair, J.R.E.; Black, W.C.; Babin, B.J. ; Anderson, Multivariate Data Analysis, 7th ed.; Pearson Educational International: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Wendt, H.W. Dealing with a common problem in Social science: A simplified rank-biserial coefficient of correlation based on the U statistic. Eur. J. Soc. Psychol. 1972, 2, 463–465. [Google Scholar] [CrossRef]
- Giezendanner, S.; Walther, S.; Razavi, N.; Van Swam, C.; Fisler, M.S.; Soravia, L.M.; Andreotti, J.; Schwab, S.; Jann, K.; Wiest, R.; et al. Alterations of white matter integrity related to the season of birth in schizophrenia: A DTI study. PLoS ONE 2013, 8, e75508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasamoto, A.; Miyata, J.; Kubota, M.; Hirao, K.; Kawada, R.; Fujimoto, S.; Tanaka, Y.; Hazama, M.; Sugihara, G.; Sawamoto, N.; et al. Global association between cortical thinning and white matter integrity reduction in schizophrenia. Schizophr. Bull. 2014, 40, 420–427. [Google Scholar] [CrossRef] [Green Version]
- Caprihan, A.; Abbott, C.; Yamamoto, J.; Pearlson, G.; Perrone-Bizzozero, N.; Sui, J.; Calhoun, V.D. Source-Based morphometry analysis of group differences in fractional anisotropy in schizophrenia. Brain Connect. 2011, 1, 133–145. [Google Scholar] [CrossRef]
- Hatton, S.N.; Lagopoulos, J.; Hermens, D.F.; Hickie, I.B.; Scott, E.; Bennett, M.R. White matter tractography in early psychosis: Clinical and neurocognitive associations. J. Psychiatry Neurosci. 2014, 39, 417–427. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Iglesias, R.; Tordesillas-Gutiérrez, D.; Barker, G.J.; McGuire, P.K.; Roiz-Santiañez, R.; Mata, I.; de Lucas, E.M.; Quintana, F.; Vazquez-Barquero, J.L.; Crespo-Facorro, B. White matter defects in first episode psychosis patients: A voxelwise analysis of diffusion tensor imaging. NeuroImage 2010, 49, 199–204. [Google Scholar] [CrossRef]
- Melicher, T.; Horacek, J.; Hlinka, J.; Spaniel, F.; Tintera, J.; Ibrahim, I.; Mikolas, P.; Novák, T.; Mohr, P.; Hoschl, C. White matter changes in first episode psychosis and their relation to the size of sample studied: A DTI study. Schizophr. Res. 2015, 162, 22–28. [Google Scholar] [CrossRef]
- Luck, D.; Buchy, L.; Czechowska, Y.; Bodnar, M.; Pike, B.; Campbell, J.S.; Achim, A.; Malla, A.; Joober, R.; Lepage, M. Fronto-Temporal disconnectivity and clinical short-term outcome in first episode psychosis: A DTI-tractography study. J. Psychiatr. Res. 2011, 45, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Szeszko, P.R.; Robinson, D.G.; Ashtari, M.; Vogel, J.; Betensky, J.; Sevy, S.; Ardekani, B.A.; Lencz, T.; Malhotra, A.K.; McCormack, J.; et al. Clinical and Neuropsychological correlates of white matter abnormalities in recent onset schizophrenia. Neuropsychopharmacology 2007, 33, 976–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneiderman, J.S.; Buchsbaum, M.S.; Haznedar, M.M.; Hazlett, E.A.; Brickman, A.M.; Shihabuddin, L.; Brand, J.G.; Torosjan, Y.; Newmark, R.E.; Canfield, E.L.; et al. Age and diffusion tensor anisotropy in adolescent and adult patients with schizophrenia. NeuroImage 2009, 45, 662–671. [Google Scholar] [CrossRef] [Green Version]
- Kyriakopoulos, M.; Perez-Iglesias, R.; Woolley, J.B.; Kanaan, R.A.A.; Vyas, N.S.; Barker, G.J.; Frangou, S.; McGuire, P.K. Effect of age at onset of schizophrenia on white matter abnormalities. Br. J. Psychiatry 2009, 195, 346–353. [Google Scholar] [CrossRef] [Green Version]
- Epstein, K.A.; Cullen, K.R.; Mueller, B.A.; Robinson, P.; Lee, S.; Kumra, S. White Matter Abnormalities and cognitive impairment in early-onset schizophrenia-spectrum disorders. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 362–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoptman, M.J.; Nierenberg, J.; Bertisch, H.C.; Catalano, D.; Ardekani, B.; Branch, C.; DeLisi, L.; Ardekani, B.A.; Branch, C.A.; DeLisi, L.E. A DTI study of white matter microstructure in individuals at high genetic risk for schizophrenia. Schizophr. Res. 2008, 106, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Boos, H.B.; Mandl, R.C.; van Haren, N.E.; Cahn, W.; van Baal, G.C.M.; Kahn, R.S.; Pol, H.E.H. Tract-Based diffusion tensor imaging in patients with schizophrenia and their non-psychotic siblings. Eur. Neuropsychopharmacol. 2013, 23, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J.I.; Tang, C.; Carpenter, D.; Buchsbaum, M.; Schmeidler, J.; Flanagan, L.; Golembo, S.; Kanellopoulou, I.; Ng, J.; Hof, P.R.; et al. Diffusion tensor imaging findings in first-episode and chronic schizophrenia patients. Am. J. Psychiatry 2008, 165, 1024–1032. [Google Scholar] [CrossRef] [PubMed]
- Mandl, R.C.W.; Schnack, H.G.; Luigjes, J.; Heuvel, M.V.D.; Cahn, W.; Kahn, R.S.; Pol, H.E.H. Tract-Based analysis of magnetization transfer ratio and diffusion tensor imaging of the frontal and frontotemporal connections in schizophrenia. Schizophr. Bull. 2010, 36, 778–787. [Google Scholar] [CrossRef] [PubMed]
- Alba-Ferrara, L.M.; de Erausquin, G.A. What does anisotropy measure? Insights from increased and decreased anisotropy in selective fiber tracts in schizophrenia. Front. Integr. Neurosci. 2013, 7, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, N.; Sakurai, T.; Davis, K.L.; Buxbaum, J.D. Linking oligodendrocyte and myelin dysfunction to neurocircuitry abnormalities in schizophrenia. Prog. Neurobiol. 2011, 93, 13–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hakak, Y.; Walker, J.R.; Li, C.; Wong, W.H.; Davis, K.L.; Buxbaum, J.; Haroutunian, V.; Fienberg, A.A. Genome-Wide expression analysis reveals dysregulation of myelination-related genes in chronic schizophrenia. Proc. Natl. Acad. Sci. USA 2001, 98, 4746–4751. [Google Scholar] [CrossRef] [Green Version]
- Fields, R.D. White matter in learning, cognition and psychiatric disorders. Trends Neurosci. 2008, 31, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Duncan, G.W.; Firbank, M.J.; Yarnall, A.; Khoo, T.K.; Brooks, D.; Barker, R.A.; Burn, D.; O’Brien, J. Gray and white matter imaging: A biomarker for cognitive impairment in early Parkinson’s disease? Mov. Disord. 2015, 31, 103–110. [Google Scholar] [CrossRef]
- Haghshomar, M.; Dolatshahi, M.; Sherbaf, F.G.; Moghaddam, H.S.; Shandiz, M.S.; Aarabi, M.H. Disruption of inferior longitudinal fasciculus microstructure in parkinson’s disease: A systematic review of diffusion tensor imaging studies. Front. Neurol. 2018, 9, 598. [Google Scholar] [CrossRef]
- Schmidt, A.; Lenz, C.; Smieskova, R.; Harrisberger, F.; Walter, A.; Riecher-Rössler, A.; Simon, A.; Lang, U.E.; McGuire, P.; Fusar-Poli, P.; et al. Brain diffusion changes in emerging psychosis and the impact of state-dependent psychopathology. Neurosignals 2015, 23, 71–83. [Google Scholar] [CrossRef]
- Tu, S.; Leyton, C.E.; Hodges, J.R.; Piguet, O.; Hornberger, M. Divergent Longitudinal propagation of white matter degradation in logopenic and semantic variants of primary progressive aphasia. J. Alzheimer’s Dis. 2015, 49, 853–861. [Google Scholar] [CrossRef] [Green Version]
- Orellana, G.; Slachevsky, A. Executive functioning in schizophrenia. Front. Psychiatry 2013, 4, 35. [Google Scholar] [CrossRef] [Green Version]
- Dong, D.; Wang, Y.; Chang, X.; Luo, C.; Yao, D. Dysfunction of large-scale brain networks in schizophrenia: A meta-analysis of resting-state functional connectivity. Schizophr. Bull. 2017, 44, 168–181. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, P.; Cappucciati, M.; Borgwardt, S.; Woods, S.W.; Addington, J.; Nelson, B.; Nieman, D.; Stahl, D.; Rutigliano, G.; Riecher-Rössler, A.; et al. Heterogeneity of psychosis risk within individuals at clinical high risk. JAMA Psychiatry 2016, 73, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Bloemen, O.J.N.; de Koning, M.B.; Schmitz, N.; Nieman, D.H.; Becker, H.E.; de Haan, L.; Dingemans, P.; Linszen, D.H.; van Amelsvoort, T.A.M.J. White-Matter markers for psychosis in a prospective ultra-high-risk cohort. Psychol. Med. 2009, 40, 1297–1304. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, P.; Prats-Galino, A.; Gallardo-Pujol, D.; Villoslada, P.; Falcón, C.; Prčkovska, V. Evaluating structural connectomics in relation to different Q-space sampling techniques. Med. Image Comput. Comput. Assist. Interv. 2013, 671–678. [Google Scholar] [CrossRef]
- Vos, S.B.; Jones, D.K.; Viergever, M.A.; Leemans, A. Partial volume effect as a hidden covariate in DTI analyses. NeuroImage 2011, 55, 1566–1576. [Google Scholar] [CrossRef]
- Kamali, A.; Flanders, A.E.; Brody, J.; Hunter, J.V.; Hasan, K.M. Tracing superior longitudinal fasciculus connectivity in the human brain using high resolution diffusion tensor tractography. Brain Struct. Funct. 2014, 219, 269–281. [Google Scholar] [CrossRef]
- Dell’Acqua, F.; Scifo, P.; Rizzo, G.; Catani, M.; Simmons, A.; Scotti, G.; Fazio, F. A modified damped Richardson–Lucy algorithm to reduce isotropic background effects in spherical deconvolution. NeuroImage 2010, 49, 1446–1458. [Google Scholar] [CrossRef]
- Clark, K.A.; Nuechterlein, K.H.; Asarnow, R.F.; Liberty, S.H.; Phillips, O.R.; Hageman, N.S.; Woods, R.P.; Alger, J.R.; Toga, A.W.; Narr, K.L. Mean diffusivity and fractional anisotropy as indicators of disease and genetic liability to schizophrenia. J. Psychiatr. Res. 2011, 45, 980–988. [Google Scholar] [CrossRef] [Green Version]
- de Weijer, A.; Mandl, R.; Diederen, K.; Neggers, S.; Kahn, R.; Pol, H.H.; Sommer, I. Microstructural alterations of the arcuate fasciculus in schizophrenia patients with frequent auditory verbal hallucinations. Schizophr. Res. 2011, 130, 68–77. [Google Scholar] [CrossRef] [Green Version]
- Abdul-Rahman, M.F.; Qiu, A.; Woon, P.S.; Kuswanto, C.; Collinson, S.L.; Sim, K. Arcuate fasciculus abnormalities and their relationship with psychotic symptoms in schizophrenia. PLoS ONE 2012, 7, e29315. [Google Scholar] [CrossRef]
- Keefe, R.S.E. The longitudinal course of cognitive impairment in schizophrenia: An examination of data from premorbid through posttreatment phases of illness. J. Clin. Psychiatry 2014, 75, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Ventura, J.; Thames, A.D.; Wood, R.C.; Guzik, L.H.; Hellemann, G.S. Disorganization and reality distortion in schizophrenia: A meta-analysis of the relationship between positive symptoms and neurocognitive deficits. Schizophr. Res. 2010, 121, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CS | FEP | UHR | |
|---|---|---|---|
| ↓FA | SLF, ILF, IFOF, CB, CC, UF, AF, IC, fornix, corona radiata, temporal lobe, occipital lobe, frontal lobe | SLF, ILF, IFOF, CC, UF, temporal lobe, parietal lobe, left frontal lobe | SLF, ILF, IFOF, CB, CC, UF, PTR, ATR, EC, IC, forceps minor, temporal lobe, frontal lobe |
| ↑FA | Right frontal lobe, left occipital lobe, insula, IC, cerebellum, inter-hemispheric and cortico-cortical tracts | SLF, IFOF, UF, AF, ATR, forceps minor, frontal lobe, right fornix |
| Ultra-High Risk Individuals (UHR) (n = 12) | First-Episode Psychosis Patients (FEP) (n = 20) | Chronic Schizophrenia Patients (CS) (n = 54) | Healthy Control (HC) (n = 33) | F/H/χ2 | |
|---|---|---|---|---|---|
| Age: M (SD) | 25.08 (4.81) | 27.00 (5.43) | 38.39 (6.64) | 37.09 (8.08) | 23.54 a,*** |
| Sex: female/male | 6/6 | 13/7 | 23/31 | 20/13 | 4.27 c |
| Antipsychotic medications: | |||||
| Atypical: n (%) | 6 (50.00) | 16 (80.00) | 33 (61.12) | - | 31.77 c,*** |
| Atypical and typical: n (%) | 0 (0.00) | 2 (10.00) | 17 (31.48) | - | |
| Typical: n (%) | 0 (0.00) | 1 (5.00) | 2 (3.70) | - | |
| No medications: n (%) | 6 (50.00) | 1 (5.00) | 2 (3.70) | - | |
| Chlorpromazine equivalent (mg): M (SD) | 131.58 (226.08) | 504.90 (336.89) | 632.09 (317.07) | - | 21.35 b,*** |
| Duration of illness: M (SD) | 1.07 (1.41) | 0.39 (0.39) | 15.18 (5.64) | - | 60.54 b,*** |
| Exacerbation: M (SD) | 4.08 (5.85) | 1.10 (0.31) | 6.37 (4.51) | - | 43.04 b,*** |
| Global functioning in GAF: M (SD) | 63.67 (14.20) | 59.65 (17.25) | 57.58 (15.24) | - | 0.77 a |
| Ultra-High Risk Individuals (UHR) (n = 12) | First-Episode Psychosis Patients (FEP) (n = 20) | Chronic Schizophrenia Patients (CS) (n = 54) | Z | |
|---|---|---|---|---|
| Positive Symptoms in PANSS: M (SD) | - | 11.40 (5.27) | 7.59 (3.54) | −3.04 * |
| Negative Symptoms in PANSS: M (SD) | - | 14.60 (5.40) | 16.81 (6.57) | −1.33 |
| Disorganization in PANSS: M (SD) | - | 13.85 (4.57) | 11.69 (3.47) | −1.89 |
| Affect in PANSS: M (SD) | - | 9.95 (3.89) | 8.67 (3.39) | −1.51 |
| Resistance in PANSS: M (SD) | - | 5.85 (2.21) | 4.61 (1.09) | −2.34 |
| Positive Symptoms in SIPS: M (SD) | 5.83 (3.90) | - | - | - |
| Negative Symptoms in SIPS: M (SD) | 10.33 (6.09) | - | - | - |
| Disorganization in SIPS: M (SD) | 3.83 (2.94) | - | - | - |
| General Symptoms in SIPS: M (SD) | 7.42 (4.01) | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waszczuk, K.; Tyburski, E.; Rek-Owodziń, K.; Plichta, P.; Rudkowski, K.; Podwalski, P.; Bielecki, M.; Mak, M.; Bober, A.; Misiak, B.; et al. Relationship between White Matter Alterations and Pathophysiological Symptoms in Patients with Ultra-High Risk of Psychosis, First-Episode, and Chronic Schizophrenia. Brain Sci. 2022, 12, 354. https://doi.org/10.3390/brainsci12030354
Waszczuk K, Tyburski E, Rek-Owodziń K, Plichta P, Rudkowski K, Podwalski P, Bielecki M, Mak M, Bober A, Misiak B, et al. Relationship between White Matter Alterations and Pathophysiological Symptoms in Patients with Ultra-High Risk of Psychosis, First-Episode, and Chronic Schizophrenia. Brain Sciences. 2022; 12(3):354. https://doi.org/10.3390/brainsci12030354
Chicago/Turabian StyleWaszczuk, Katarzyna, Ernest Tyburski, Katarzyna Rek-Owodziń, Piotr Plichta, Krzysztof Rudkowski, Piotr Podwalski, Maksymilian Bielecki, Monika Mak, Adrianna Bober, Błażej Misiak, and et al. 2022. "Relationship between White Matter Alterations and Pathophysiological Symptoms in Patients with Ultra-High Risk of Psychosis, First-Episode, and Chronic Schizophrenia" Brain Sciences 12, no. 3: 354. https://doi.org/10.3390/brainsci12030354